
Stryker and Gauss Surgical – Case Study
With more than 50 acquisitions in the past decade, Stryker has not been coy about the company’s desire to increase the pace of mergers and acquisitions (M&As) in 2024. Over this period, some of these acquisitions have drawn major industry attention (and even criticism). Other deals include smaller “tuck-ins,” which make up most of the volume of the company’s M&As. These often occur with less industry fanfare.
Some of these tuck-in acquisitions make sense. Cerus Endovascular fits nicely into the company’s $1.2B Neurovascular business. The March 2024 acquisition of French-based joint replacement company SERF SAS boosts Stryker’s global presence and will contribute to increased growth in the company’s $2.3B and $1.5B knee and hip businesses, respectively.
Then, there are the acquisitions that have attracted tremendous attention in the medtech industry. Many critical articles were written about Stryker’s $1.65 billion acquisition of Mako. In retrospect, the acquisition has been seen as a success that has since bolstered Stryker’s position in both the hip and knee implants market.
Robotics have been and continue to be a source of fascination in the medical industry. There is something that inspires awe in us when we consider the idea of robots performing operations on humans. However, if one looks practically at the technology, it can be stated that robotic systems purportedly save the healthcare system money, reduce the burden on healthcare providers, and improve patient quality of life.
So why do some acquisitions get less attention than others? Take, for example, Stryker’s September 2021 acquisition of Gauss Surgical for $120 million in upfront cash plus an additional $40 million in milestone payments. The details and outcomes of this transaction did not draw nearly as much attention as the acquisition of Mako did.
Perhaps it is easy to understand why. Gauss Surgical developed and commercialized Triton, a real-time solution to monitor blood loss during surgery. The device utilizes artificial intelligence to quickly quantify blood loss and indicate the possibility of a hemorrhage. If we return to the practical examination on robotic systems, we see that Stryker acquired a device that purports to save the healthcare system money, reduces the burden on healthcare providers, improves patient quality of life, and prevents morbidity.
At face value, this acquisition is certainly less exciting than a surgeon-controlled robot replacing a knee.
The Global Burden of Major Bleeding Complications in Surgery
Consider that hundreds of millions of patients undergo surgery each year.1 In many of these operations, major bleeding is a common complication.2 Major bleeding is one of the most common, if not the most common, surgical complication.
For example, a study by Spence et al. (2019) looked at 40,004 patients in 14 countries who underwent noncardiac surgery. Of these, the most common major complication was major bleeding, which was seen in 6,238. The study found that major bleeding resulted in 361 deaths within the first 30 days post-surgery. This translated to approximately 5.8% of patients who experienced major bleeding dying. Other major complications included myocardial injury after noncardiac injury and sepsis.
Overall, the study by Spence et al. (2019) found that 1.8% of noncardiac surgeries died within 30 days of surgery. Assuming that worldwide, 300 million patients undergo surgery, and 1.8% of them die within 30 days of surgery, this translates to 5.4M deaths each year. If we look at major bleeding alone – 15.6% of 300M is 46.8M major bleeding incidents. Using this study’s findings, which estimate that 5.8% of those patients will then die within 30 days due to the major bleeding event, approximately 2.7M patients die each year due to major bleeding complications. This is a substantial global health problem in need of modern solutions to address.
Other studies by Freundlich et al. (2019), Roshanov et al. (2021), and Roshanov et al. (2024) confirm the significant burden that major bleeding complications present in most forms of surgery.
Current Methods and Innovations in Monitoring Major Bleeding
So, what is currently being done to monitor for indications of major bleeding?
There are three primary methods in which blood loss is quantified during and after surgery.7,8,9
-
Visual estimation
-
The gravimetric method
-
Lab testing
By most accounts, visual estimation is the standard of care for determining blood loss. It involves a visual assessment of the surgical fluid combined with the collection of fluids, including bile, irrigation fluids, lymph and other fluids combined with lost blood. It is widely regarded as inaccurate and unreliable.
The popularity of the visual estimation approach is likely due to its ease-of-use and its compatibility with supporting methods to assess blood loss (e.g., vital signs monitoring, laboratory metrics). Despite being well studied and perceived as inaccurate, it is the most common method for determining estimated blood loss (EBL).
The gravimetric method involves the weighing of surgical sponges before and after surgery. EBL is assessed based on the difference in weight. It is also inaccurate due to the inclusion of the accumulation of the aforementioned fluids found in the operating room.
Laboratory testing and photometric (i.e., spectrophotometry) analysis have been discussed as potential “gold standard” approaches for quantifying blood loss. These approaches quantify hemoglobin concentration. When hemoglobin falls below a threshold – typically 6 to 7 g/dL – the clinical team needs to intervene. While these approaches are more accurate, they also are more costly, laborious, and time-consuming.10
Gauss Surgical recognized a significant unmet need in the management of surgical patients. The company’s Triton System analyzes real-time images of surgical sponges and suction canisters with an image analysis algorithm that estimates hemoglobin mass. To the credit of Gauss Surgical, the company has obtained clinical data supporting the benefits of adopting their technology when compared to visual and gravimetric estimation.
To date, Triton is largely marketed and utilized as a solution for maternal hemorrhage care. While maternal hemorrhage carries significant mortality risks to women, it captures only a subset of patients who are at risk of death due to major bleeding complications. The narrow focus on OB/GYN procedures ignores approximately 10M US-based procedures and 37M procedures performed globally that could benefit from accurate quantification of blood loss to improve peri- and postoperative patient care.11
There are few alternatives to Triton in the competitive landscape for other device-based approaches for detecting major blood loss. As part of this analysis, LSI searched for alternative solutions being developed and commercialized for quantifying blood loss. Many of the technologies identified are still in the preclinical stage.
Stryker’s Instruments Innovation Sensor is evaluating, in the preclinical setting, a device that utilizes optical analysis to measure the hemoglobin concentration of fluid mixtures. The optical module, referred to as the Stryker system, integrates within a liquid waste management system. Results of the study found the device to be commensurable with the performance of hematology analyzers.12
Cypher Medical has developed a solution to continuously monitor red blood cell (RBC) sedimentation during surgical procedures. It is purported to integrate into existing blood and fluid management systems, providing a cost-effective and simple solution to quantify blood loss. Cypher Medical utilizes a proprietary liquid chemical agent to force RBC to separate from collected intraoperative fluids. The solution provides the surgical team with a solution to quantify red blood cells without the need for laboratory tests or additional equipment.
A pilot study evaluated the ThermaSense AccuFlow sensor as a novel tool to detect hemorrhage in surgical settings. Compared to other technological approaches, the AccuFlow sensor focuses on monitoring perfusion measurements for early signs of hemorrhage.13
LSI identified one company, Ecomed Solutions, that offers HEMAsavR, a blood management device that is compatible with current surgical waste management and autotransfusion systems. The device collects blood for cell salvage processing to facilitate autotransfusion and provides the surgical team with enhanced visualization and tracking of blood loss through measurements on the side of the collection canister.
The Economic and Clinical Impact of Accurate Blood Loss Monitoring
This analysis has already explored the most obvious problem that remains unmanaged – the mortality associated with major bleeding complications. There are other considerations intrinsically tied to monitoring blood loss. Fluid management, blood transfusion and pharmacologic intervention (e.g., thromboprophylaxis) decisions, and predicting postoperative outcomes are all tied to understanding blood loss. These decisions involve additional costs – both financial and outcomes-related.
In a single-center study conducted by Gauss Surgical in 2019, annualized direct cost savings of $209,228 were recognized from the implementation of a more effective solution for quantifying blood loss. Of these, $172,614 was saved from laboratory costs and $36,614 from blood bank (i.e., transfusion) costs. The study builds on previous research that shows that when compared to visual estimation, Triton improves the recognition of hemorrhages, reduces unnecessary transfusions, and shortens hospital stays.
Considering that the most widely employed methods for EBL are inaccurate, there is an overreliance on blood transfusions. Some studies have estimated that approximately 40 to 45% of transfusions could be unnecessary.15 Other studies indicate that 22 to 57% of transfusions could be inappropriate.16
There are significant costs associated with unnecessary blood transfusion. Patients can experience adverse reactions to the transfusion (e.g., infections) and organ injury (e.g., acute lung injury). Blood transfusions are also associated with increased length of stay.16 Conservative blood use programs are widely recommended. These programs are dependent on education, policy changes, decision support systems, and audits to reduce rates of unnecessary blood transfusions. In 2016, the Joint Commission and the Association for the Advancement of Blood and Biotherapies (AABB) developed a voluntary Patient Blood Management (PBM) program for US hospitals.
Perhaps of most interest to hospital administrators today is the cost associated with reducing unnecessary transfusions. The average units of blood per transfusion is 3.17 The overall cost to provide a RBC transfusion ranges from $522 to $1,183, with annual expenditures on blood limited to surgical patients ranging from $1.62M to $6.03M per hospital (Shander et al., 2010). Assuming 40% of transfusions are unnecessary, this translates to $0.65M to $2.4M in unnecessary spending per hospital.
Furthermore, there is a correlation between increased length of stay (LOS) and blood transfusion. Many studies across surgical disciplines have found that patients who receive a blood transfusion stay in the hospital longer.18, 19, 20, 21, 22, 15, 23
An analysis conducted in 2016 by the Agency for Healthcare Research and Quality compared 1.1M and 2.1M hospital stays in 2000 and 2013, respectively. In patients who received an RBC transfusion, the mean length of stay was 8.9 days in 2000 and 8.3 days in 2013. By comparison, the mean LOS among adults was 4.9 days in 2000 and 4.7 days in 2013. The LOS for patients who received a transfusion appears to have increased according to data published by the Joint Commission in 2022.24, 15
The per inpatient day cost in the US ranges from $2,296 to $3,013.25, 26, 27 Multiple sources agree that the average inpatient day cost is $2,883. The average LOS is 4.6 days at an average cost of $13,262.25 That same average cost for a patient who receives an RBC transfusion is $24,794 for an 8.6 day stay. An 87% increase.
According to LSI’s Global Surgical Procedure Volumes database, we estimate that there are approximately 13M high-risk blood loss procedures performed annually in the US. If we assume that 40% of these procedures receive an inappropriate blood transfusion due to poor ability to quantify blood loss, then approximately 5.2M procedures are performed with an unnecessary blood transfusion. These patients, on average, will stay in the hospital for 8.6 days for a total of 44.72M patient days. Continuing with the assumption that the average inpatient day costs $2,883, this equates to $129B in hospital spending.
Estimate on Indirect Spending for Unnecessary Blood Transfusions in the US
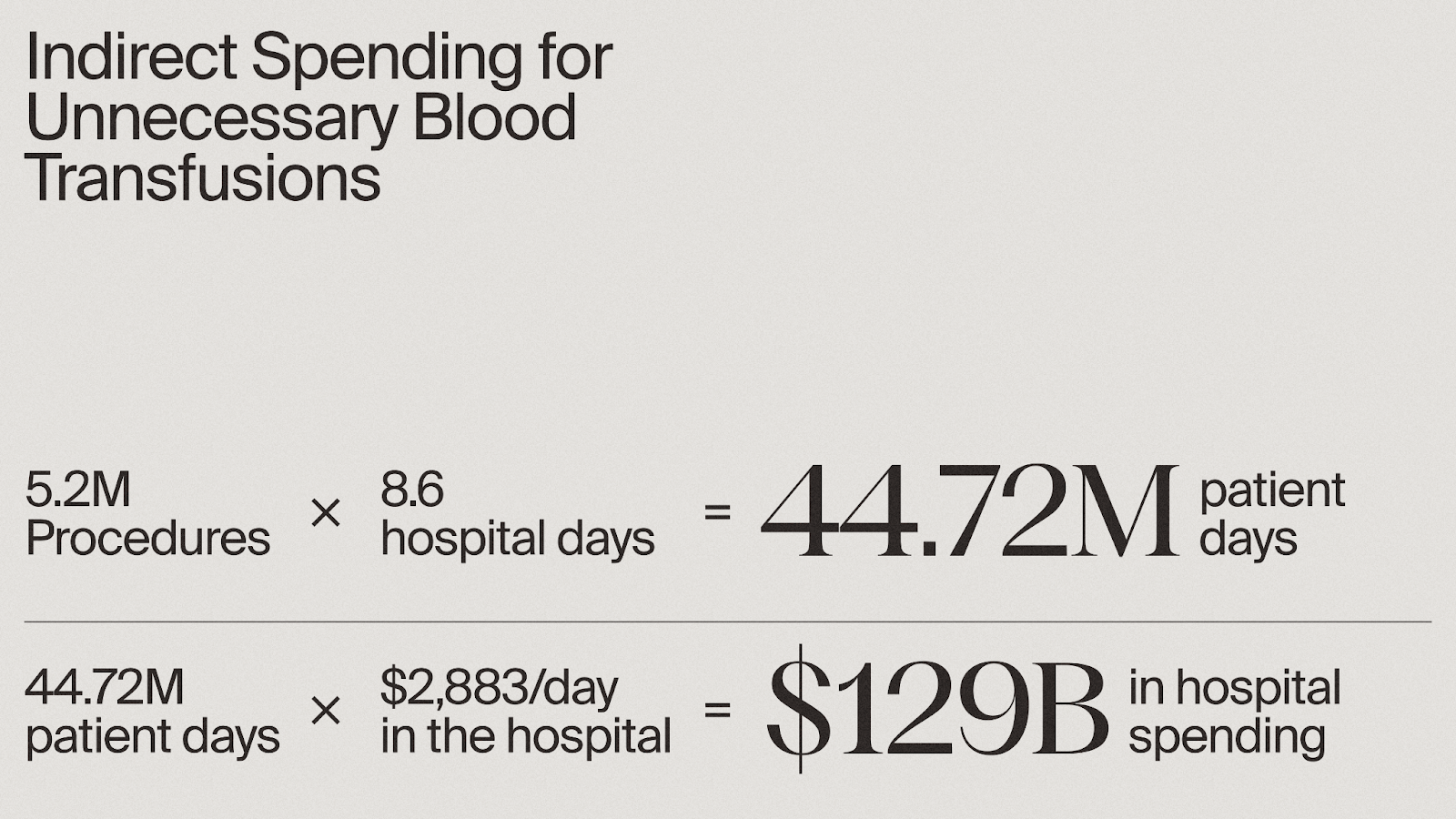
It can be confidently stated that programs and solutions to reduce unnecessary transfusions could significantly reduce procedure and total hospital costs.
Addressing the Global Health Burden of Major Bleeding: Challenges and Opportunities
This analysis shows that blood loss is a significant cause of mortality (~3M deaths per year worldwide) and carries steep costs for healthcare. In the absence of a gold standard to monitor intraoperative blood loss, it is likely that healthcare providers will continue to use inaccurate methods to estimate blood loss and perform unnecessary transfusions based on these dubious estimates.
It’s worth stating that this analysis focused only on procedures that are known for being at increased risk of major bleeding complications and, therefore, more subject to the errors and complications associated with major bleeding risk. The clinical literature and other secondary sources accessed for this analysis agree that blood transfusion is one of the most performed procedures in the hospital. Why?
Even procedures with a lower risk of major bleeding complications need to monitor blood loss to ensure the patient remains stable. The need for accurate quantification of blood loss is agnostic of procedure risk; therefore, hundreds of millions of procedures performed worldwide could benefit from better technologies and policies to improve intraoperative blood loss monitoring.
Gauss Surgical obtained FDA 510(k) approval for the Triton System in May of 2014. A decade later, Triton is still primarily marketed as a solution to address maternal hemorrhage. At the same time, hundreds of millions of surgical procedures performed each year rely on methods that are recognized for their inaccuracy in quantifying blood loss. Stryker completed its acquisition of Gauss Surgical and the Triton system in September of 2021. Despite the temporary attention raised due to a major medtech strategic making an acquisition that intended to address the global health burden of major bleeding, LSI’s review of recent clinical literature still indicates that a solution to improve intraoperative blood loss and reduce costs associated with major bleeding has yet to be found.
Initiatives have been taken to improve education, policy, and clinical decision-making to reduce transfusions while seemingly ignoring the reality that faulty methods are in place prior to a decision to transfuse. It remains clear that there is a great unmet need that addresses the global health burden of intraoperative major bleeding.
It is worth questioning why this burden does not receive more consideration.
References:
-
Shah, A., Palmer, A. J. R., & Klein, A. A. (2020). Strategies to minimize intraoperative blood loss during major surgery. British Journal of Surgery, 107(2), e26–e38. https://doi.org/10.1002/bjs.11393
-
Halme, A. et al (2024). Timing of Major Postoperative Bleeding Among Patients Undergoing Surgery. JAMA Netw Open. 2024;7(4):e244581. doi:10.1001/jamanetworkopen.2024.4581.
-
Spence, J. et al (2019). Association between complications and death within 30 days after noncardiac surgery. CMAJ. 2019 Jul 29; 191(30): E830–E837. doi:10.1503/cmaj.190221
-
Freundlich, R. E., Maile, M. D., Sferra, J. J., Jewell, E. S., Kheterpal, S., & Engoren, M. (2018). Complications Associated With Mortality in the National Surgical Quality Improvement Program Database. Anesthesia and analgesia, 127(1), 55–62. https://doi.org/10.1213/ANE.0000000000002799
-
Roshanov, P.S. et al. (2021) Bleeding Independently associated with Mortality after noncardiac Surgery (BIMS): an international prospective cohort study establishing diagnostic criteria and prognostic importance. British Journal of Anaesthesia, 126(1), 163-171. https://doi.org/10.1016/j.bja.2020.06.051.
-
Roshanov, P.S. et al. (2024) One-year Outcomes after Discharge from Noncardiac Surgery and Association between Predischarge Complications and Death after Discharge: Analysis of the VISION Prospective Cohort Study. Anesthesiology 2024; 140:8–24 doi: https://doi.org/10.1097/ALN.0000000000004763
-
Gerdessen, L., Meybohm, P., Choorapoikayil, S., et al. (2021) Comparison of common perioperative blood loss estimation techniques: a systematic review and meta-analysis. Journal of Clinical Monitoring and Computing; 35, 245-258.
-
Zajak, J., Páral, J., Sirový, M. et al. (2024) Blood loss quantification during major abdominal surgery: prospective observational cohort study. BMC Surg 24, 5. https://doi.org/10.1186/s12893-023-02288-w.
-
Tran, A., Heuser, J., Ramsay, T., et al. (2021). Techniques for blood loss estimation in major non-cardiac surgery: a systematic review and meta-analysis. Canadian Journal of Anesthesia; 68: 245-255.
-
Sharareh, B., Woolwine, S., Satish, S., Abraham, P., & Schwarzkopf, R. (2015). Real Time Intraoperative Monitoring of Blood Loss with a Novel Tablet Application. The open orthopaedics journal, 9, 422–426. https://doi.org/10.2174/1874325001509010422
-
Life Science Intelligence (2024). Global surgical procedure volumes database. https://www.lifesciencemarketresearch.com/procedure-volumes
-
Lufti, A., Eustace, D., Faul, S., et al. (2024). Accuracy testing of a novel obstetric blood loss quantifying device: a pilot study. International Journal of Gynecology & Obstetrics; 165(3), 1290-1292. https://doi.org/10.1002/ijgo.15385
-
Lord, M., Gould, A., Clark, M., Rouse, D. & Lewkowitz, A. (2023). The AccuFlow sensor: a novel digital health tool to assess intrapartum blood loss at cesarean delivery. Journal of Perinatal Medicine, 51(8), 997-1005. https://doi.org/10.1515/jpm-2023-0101
-
Memorial Care Innovation Fund (2019). New publication concludes Gauss Surgical’s Triton system associated with improved outcomes and reduced costs. https://memorialcareinnovationfund.com/new-publication-concludes-gauss-surgicals-triton-system-associated-with-improved-outcomes-and-reduced-costs/
-
Jadwin, D. F., Fenderson, P.G., Friedman, M.T., et al. (2022). Determination of Unnecessary Blood Transfusion by Comprehensive 15-Hospital Record Review. The Joint Commission Journal on Quality and Patient Safety; 49(1), 42-52. https://doi.org/10.1016/j.jcjq.2022.10.006.
-
Mehta, N., Murphy, M.F., Kaplan, L., Levinson, W. (2021) Reducing unnecessary red blood cell transfusion in hospitalized patients. BMJ 2021; 373, n830. https://doi.org/10.1136/bmj.n830
-
Furst, Jay (2021) Comprehensive patient blood management program can reduce use of transfusions, improve patient outcomes. https://newsnetwork.mayoclinic.org/discussion/comprehensive-patient-blood-management-program-can-reduce-use-of-transfusions-improve-patient-outcomes/
-
American Red Cross. Importance of the blood supply. https://www.redcrossblood.org/donate-blood/how-to-donate/how-blood-donations-help/blood-needs-blood-supply.html
-
Galas, Filomena & Almeida, Juliano & Fukushima, Julia & Osawa, Eduardo & Nakamura, Rosana & Silva, Carolina & Almeida, Elisângela & Auler, José & Vincent, Jean-Louis & Hajjar, Ludhmila. (2013). Blood transfusion in cardiac surgery is a risk factor for increased hospital length of stay in adult patients. Journal of cardiothoracic surgery. 8. 54. 10.1186/1749-8090-8-54.
-
Hajjar, L., Vincent, J. L., Almeida, J., Jatene, F., Rodrigues, A., Fukushima, J., Nakamura, R., Silva, C., Osawa, E., Kalil, R., Galas, F., & Auler, J., Jr (2012). Blood transfusion after cardiac surgery increases the hospital length of stay in adult patients. Critical Care, 16(Suppl 1), P447. https://doi.org/10.1186/cc11054.
-
Bou Monsef, J., & Boettner, F. (2014). Blood management may have an impact on length of stay after total hip arthroplasty. HSS journal : the musculoskeletal journal of Hospital for Special Surgery, 10(2), 124–130. https://doi.org/10.1007/s11420-014-9384-x
-
Schneider, A, M., Denyer, S., Brown, N. M., (2021). Risk factors associated with extended length of hospital stay after geriatric hip fracture. JAAOS: Global Research and Reviews 5(5):p e21.00073. DOI: 10.5435/JAAOSGlobal-D-21-00073
-
Liu, Z.Q., Wu, H.X., Cheng, S. et al. (2020). Unnecessary blood transfusion prolongs length of hospital stay of patients who undergo free fibular flap reconstruction of mandibulofacial defects: a propensity score – match study. Journal of Oral and Maxillofacial Surgery; 78(12), 2316-2327. https://doi.org/10.1016/j.joms.2020.07.213
-
Qi, Q., Qian, X., Zhu, X., et al. (2021). Perioperative transfusion is related to the length of hospital stays in primary liver cancer patients. Cancer Manag Res; 13, 4947-4954 https://doi.org/10.2147/CMAR.S296022
-
West, K.A., Barrett, M.L., Moore, B.J., et al. (2016). Trends in hospitalizations with a red blood cell transfusion, 2000-2013. https://hcup-us.ahrq.gov/reports/statbriefs/sb215-Red-Blood-Cell-Transfusions-Trends.jsp#:~:text=22.020$23%2C300
-
Gamble, Molly (2023). Hospital expenses per inpatient day across 50 days. https://www.beckershospitalreview.com/finance/hospital-expenses-per-inpatient-day-across-50-states-2023.html
-
Milliken, Maureen (2023). Hospital and surgery costs. https://www.debt.org/medical/hospital-surgery-costs/
-
Hartwick, Preston (2024). A night to remember: the staggering costs of a single hospital stay revealed. https://finance.yahoo.com/news/night-remember-staggering-costs-single-190018622.html






© 2026 Life Science Intelligence, Inc., All Rights Reserved. | Privacy Policy | Your Privacy Choices | Delete my Data